
Clinical Results
Hypertension Program Results
MHM’s hypertension cohort comprised patients who were previously uncontrolled or only marginally controlled on existing therapy. Key metrics are summarized below.
| Metric | Result | Notes |
|---|---|---|
|
Hypertensive patients with improvement |
83 % |
Patients exhibiting a lower average systolic or diastolic pressure during the late monitoring window compared with baseline. |
|
Patients reaching target range |
63 % |
Proportion of hypertensive patients whose blood pressure readings moved into the target range defined by their physician. |
|
Patients monitored ≥6 months with lower diastolic |
81 % |
Longer enrolment resulted in greater diastolic improvement. |
|
All patients with lower diastolic pressure |
59.3 % |
Across all hypertensive patients, more than half lowered their diastolic pressure compared with baseline across all length of stay durations. |
|
Patients monitored ≥6 months with lower systolic |
71 % |
Sustained monitoring correlates with larger systolic reductions. |
|
All patients with lower systolic pressure |
57.0 % |
Over half of the cohort lowered their systolic pressure across all length of stay durations. |
|
Reduction in critical
hypertensive events/patient at 3 months
|
67.2 %
|
A comparison of critical hypertensive events rates during the first month vs. the third month shows a 67 % reduction in crisis-level episodes on a per patient basis.
|
Blood‑pressure Improvement Over Time
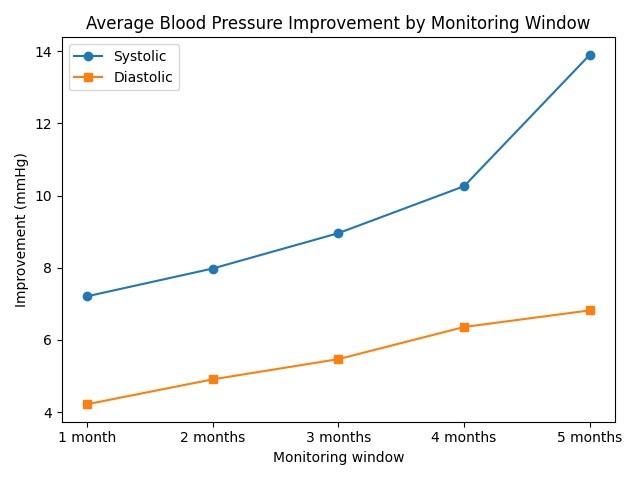
Average blood‑pressure improvements increased with the length of monitoring. After one month of RPM, patients showed a 7.21 mmHg reduction in systolic pressure and 4.22 mmHg reduction in diastolic pressure. After five months, systolic improvement reached 13.9 mmHg and diastolic improvement 6.82 mmHg, demonstrating that sustained RPM leads to progressively better control. A review of 48 randomized clinical trials found that each 5 mm Hg reduction in systolic blood pressure reduces the risk of major cardiovascular events by roughly 10 percent.
Remote patient monitoring dramatically reduced the number of crisis-level hypertensive episodes per patient. Crisis level events were defined as blood pressure exceeding 180 mm HG systolic and/or 120 mm diastolic. In the first month of monitoring, the program recorded an average of 0.32 events per patient. By the third month of service, that number fell to 0.105 critical events per patient, representing a 67 % reduction in the number of critical hypertensive events on a per patient basis. A combination of patient support and coaching, physician driven medication adjustments, and rapid identification of medication non-adherence are the primary drivers of these results, all enabled by real time physiological monitoring.
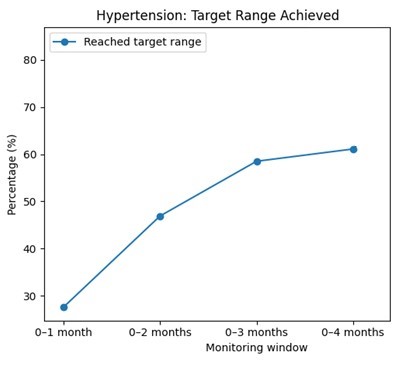
Patients reaching target range by monitoring window
The proportion of hypertensive patients reaching the target range climbed steadily with longer patient stays. Only 27.6 % of patients reached target after one month, but 61.1 % had done so by four months. We expect results to continue to improve with length of stay. These results show that sustained monitoring not only increases the percentage of patients reaching their target range, but also effectively holds patients in that range on a long-term basis.
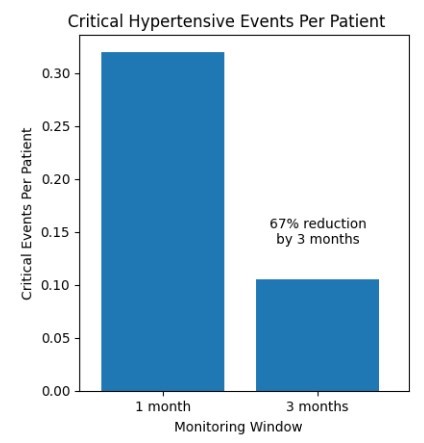
Critical Hypertensive events
Remote patient monitoring dramatically reduced the number of crisis-level hypertensive episodes per patient. Crisis level events were defined as blood pressure exceeding 180 mm HG systolic and/or 120 mm diastolic. In the first month of monitoring, the program recorded an average of 0.32 events per patient. By the third month of service, that number fell to 0.105 critical events per patient, representing a 67 % reduction in the number of critical hypertensive events on a per patient basis. A combination of patient support and coaching, physician driven medication adjustments, and rapid identification of medication non-adherence are the primary drivers of these results, all enabled by real time physiological monitoring.
Congestive Heart Failure Program Results
Heart‑failure patients were monitored primarily using connected weight scales to detect early fluid retention. Rapid gains of ≥3 lb. in 24 hours or ≥5 lb. in a week are treated as critical alerts and trigger immediate RN triage and Physician escalation. Patient support goes far beyond threshold breaches: clinicians continuously review all vital data and regularly speak with patients about healthy living, diet, medication adherence and exercise. This holistic approach helps detect early signs of decompensation while empowering patients to manage their heart failure proactively.
Critical Weight‑gain Events
| Monitoring window | Patients | Patients with ≥1 rapid gain (≥3 lb/24 h) | Rapid gain events | Patients with ≥1 large gain (≥5 lb/7 d) | Large gain events | Combined events per patient |
|---|---|---|---|---|---|---|
|
1 month |
71 |
34 |
74 |
28 |
62 |
1.915 |
|
2 months |
65 |
22 |
53 |
19 |
40 |
1.431 |
|
3 months |
53 |
14 |
32 |
11 |
17 |
0.925 |
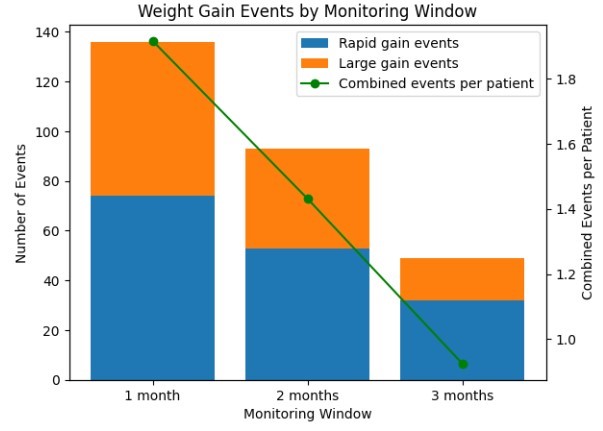
The total number of rapid and large weight‑gain events dropped sharply over time. Combined events per patient fell from 1.915 in the first month to 0.925 by month three—a 51.7 % reduction. The stacked bar chart below shows how rapid and large gain events decreased over each monitoring window, while the line illustrates the decline in combined events on an event per patient basis.
Uncontrolled heart failure is considered one of the most expensive chronic conditions. Reducing critical weight gain events on a per patient basis by 50% in a three-month period represents one of the most effective population health solutions available today from the standpoint of both reducing acute utilization costs and driving life prolonging care. In another CHF/RPM study performed by Midwest for another client, the total CHF population mean coefficient of variation (MCV) of patient weight was reduced by over 65% in 18 months and held at 2.7% or less in a sustained manner. The combination of early episode stabilization (reduction of critical weight gain events) and long-term population stabilization at t=>12 months (sustained sub-3% MCV) offers a compelling solution for modern CHF management.
Diabetes Program Results
Diabetic patients used cellular glucometers to transmit fasting and post‑prandial glucose values. Health coaches watched for hyper‑ and hypoglycemic excursions and contacted patients to confirm adherence to medications and diet.
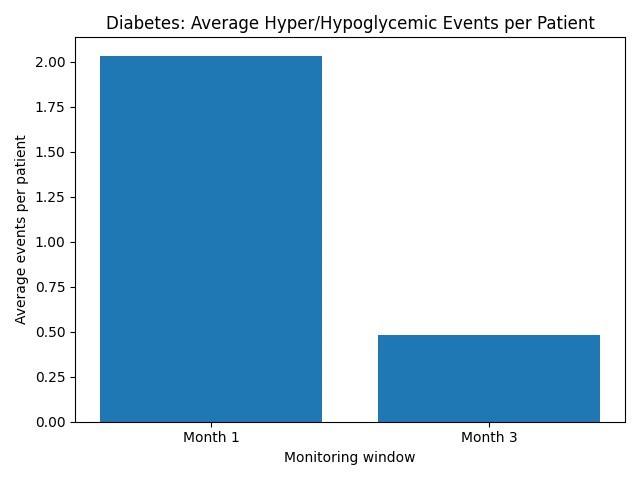
We analyzed the number of critical hyper/hypoglycemic events during the patient’s first month of service and then compared it with the number of critical hyper/hypoglycemic events in the third month of service. Providers generally consider values above 180 mg/dL to be hyperglycemia and values below 70 mg/dL to be hypoglycemia. The report grouped both hyperglycemic (>180 mg/dL) and hypoglycemic (<70 mg/dL) excursions as “crisis” events for the purpose of measuring program impact.
| Monitoring window | Average crisis hyper/hypoglycemic events per patient |
|---|---|
|
Month 1 |
2.034483 |
|
Month 3 |
0.482759 |
Within the first three months of monitoring, the average number of hyper/hypoglycemic crisis events per patient fell from 2.03 to 0.48, representing a 76.3 % reduction. The bar chart below visualizes this sharp decline. Midwest found that many of the patients in the diabetes cohort were not regularly taking their blood sugar prior to joining the program. Since Midwest provides the patient with the glucometer and monthly allotments of testing strips, the patients were able to conveniently take their readings while also benefiting from health coach support.
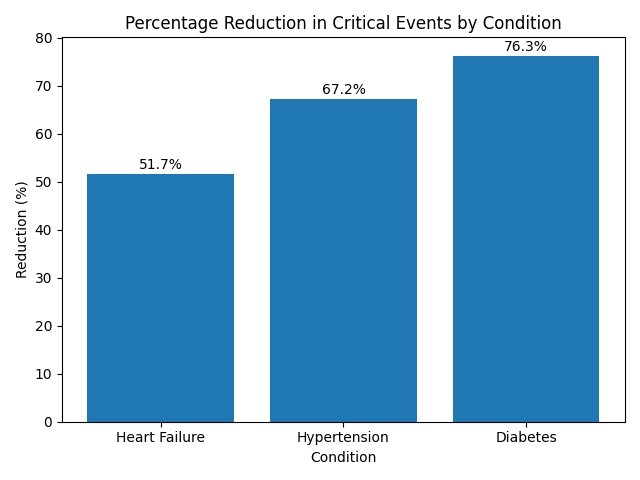
Comparative Reduction Across Conditions
Remote patient monitoring drove substantial reductions in critical events on per-patient basis across all three chronic conditions. Heart-failure patients experienced a 50% drop in crises, hypertensive patients saw an even steeper decline, and the diabetes cohort achieved the most dramatic improvement, with more than three-quarters of events avoided. Such improvements underscore how proactive monitoring and timely interventions can stabilize chronically ill populations.